

Modern waterworks and sewerage systems emerged around the world over the period 1850–1950. Today, there are gaping differences in available sanitary infrastructure. This column tracks the origins and diffusion patterns of the sanitary revolution in Colombia, Germany, the Netherlands, the UK, and the US. Piped water and sewers induced important declines in mortality but to a lower extent than thought previously due to their interaction with local contexts. More attention is needed to examine how economic and political considerations (e.g. franchise extension, construction costs) interact with broader biogeographic and cultural contexts.
Ensuring universal access to safe water and waste disposal is a key priority of the international development agenda, as highlighted by Sustainable Development Goal 6 ‘clean water and sanitation’ (United Nations 2022). This is not surprising given the gaping differences in the provision of sanitary infrastructures throughout the world. When did these inequalities emerge, and what were their health consequences? Also, what drove the unequal diffusion of waterworks and sewerage systems?
To answer these questions, we must direct our attention to the period ca. 1850–1950, when ‘modern’ systems of water supply and sewerage emerged. Although their precise impact on health outcomes has been subject to some debate (Anderson et al. 2022, Alsan and Goldin 2019, Cutler and Miller 2005), financial and political considerations are often highlighted as major obstacles to their construction (Beach et al. 2022, Brown 1988, Chapman 2022). Most of the literature, however, tends to focus on a small number of Western countries and rarely adopts a comparative perspective. This limits the generalisation of some of its findings and fails to provide a comprehensive account of the causes and consequences of the ‘sanitary revolution’.
My research fills this gap by tracking the origins and diffusion patterns of the sanitary revolution between ca. 1850 and 1940 with novel data (Gallardo-Albarrán 2024). Then, to assess their health consequences and explain their timing, I survey the economic history literature. I also draw extensively on research from economics, history, and historical demography. This exercise identifies distinct between- and within-country patterns that will raise some (unanswered) questions worth pursuing from an international and comparative perspective that the literature has missed so far.
The global diffusion of waterworks and sewerage (ca. 1850–1950)
Waterworks were established in a number of countries beyond the UK from the mid-19th century onwards. For instance, consider the waterworks construction dates in Hamburg (1849), Buenos Aires (1869), New York (1842), Bombay (1858), or St. Louis (1886). Modern sewerage systems were built around the same time, albeit with a delay that differed across places, though there are exceptions to this.
The diffusion accelerated in some countries in the 1870s, which created long-lasting diverging trends between industrialised and non-industrialised countries. Lack of standardised data makes it difficult to show this thoroughly but, to partially overcome this problem, I put together information on the timing of waterworks and sewerage systems between 1870 and 1940 from secondary sources (Table 1). The small sample considered here includes the frontrunner in sanitary matters at the time (UK), along with industrialising followers (US, Germany, and the Netherlands) and a country from the Global South (Colombia).
Table 1 Diffusion of waterworks in selected countries, 1870–1940
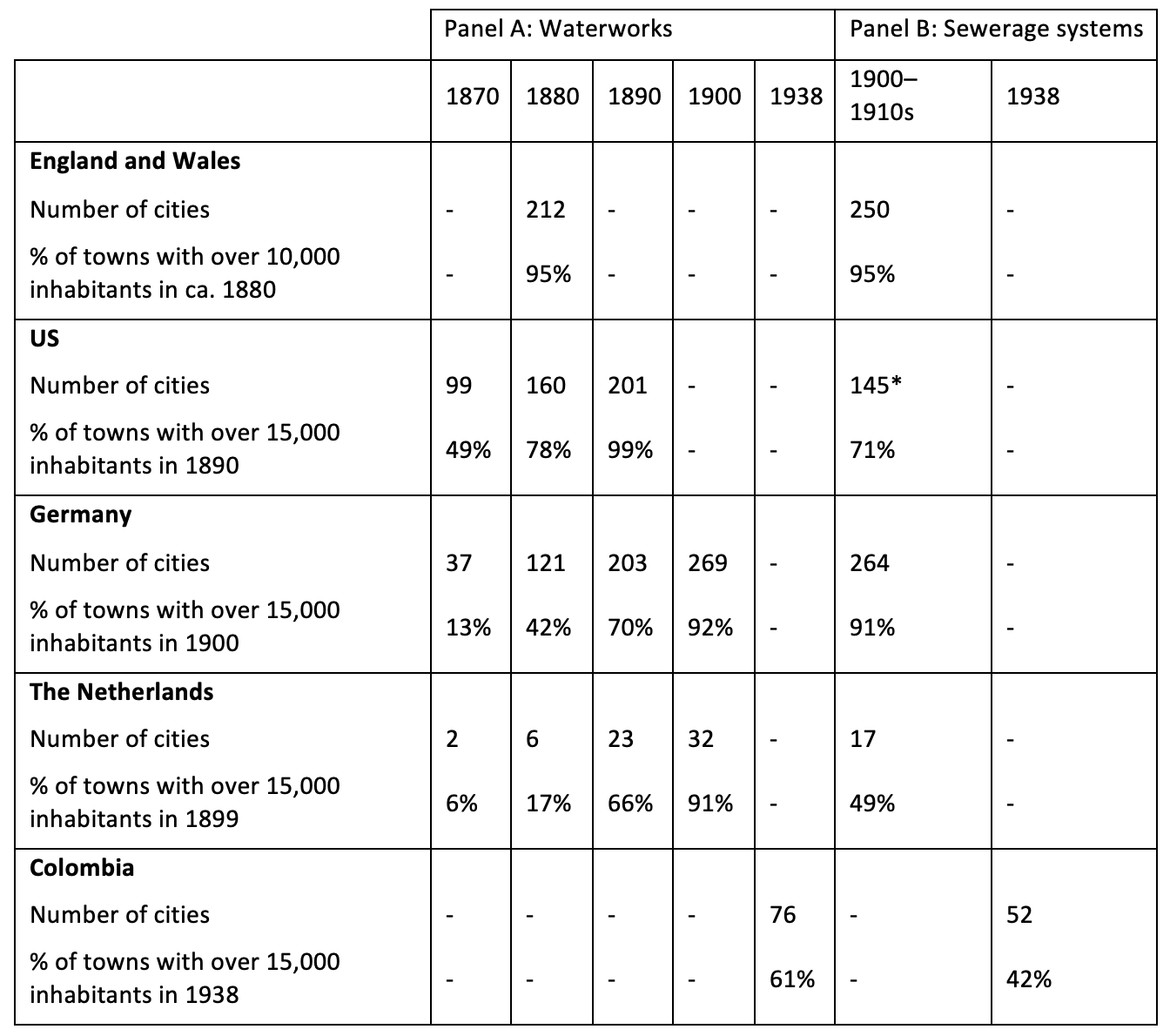
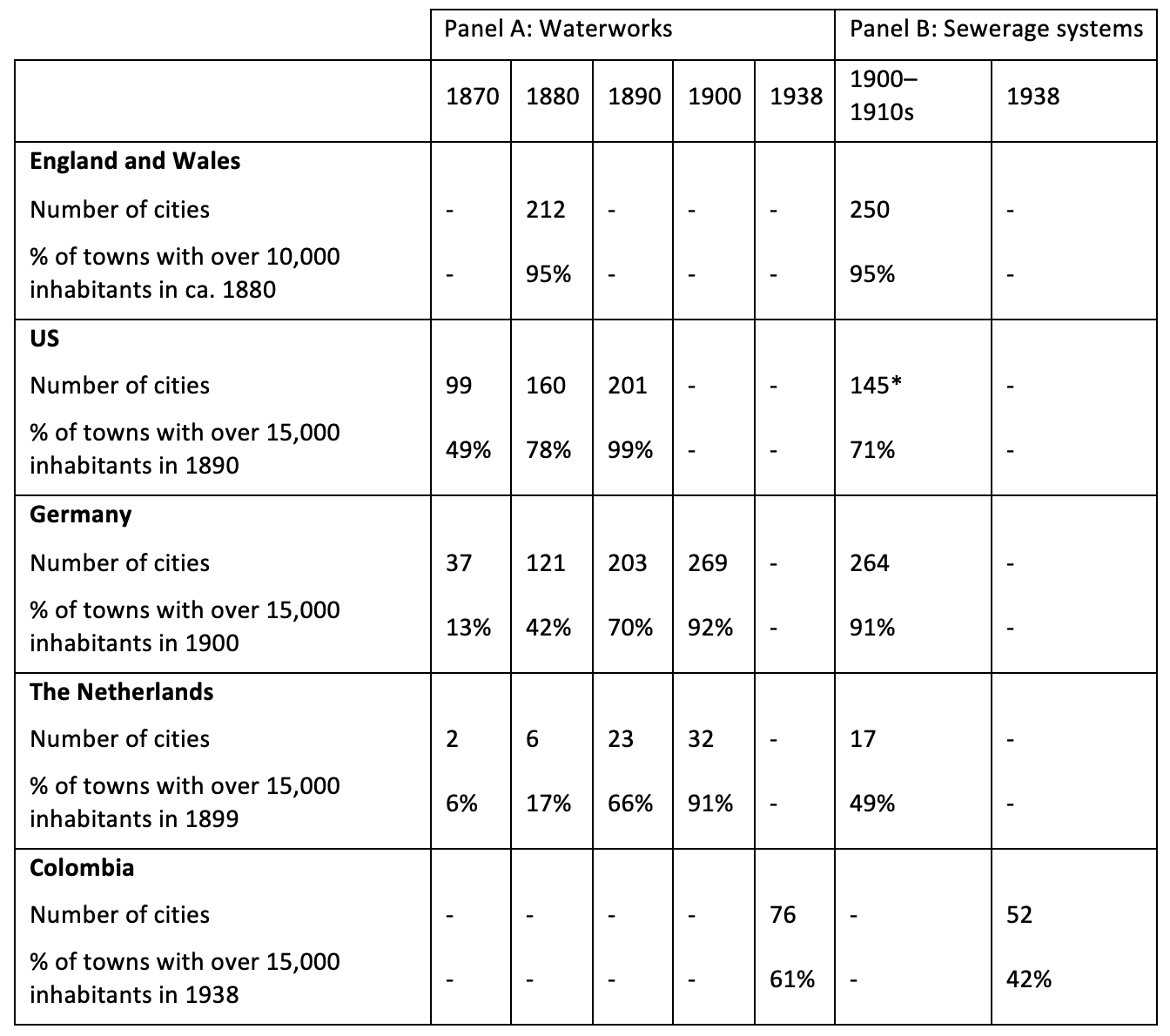
Sources: Gallardo-Albarrán (2024).
Panel A of Table 1 presents interesting patterns that partly reflect the origins of current inequalities in access to safe water. First, the UK was the indisputable leader: almost all British towns had waterworks around 1880, while the US and Germany lagged behind with coverage rates around 80% and 40%, respectively. Second, substantial investments were made from the 1870s onwards, although the pace of progress was uneven between countries. In the group of industrialising economies, we see that Germany lagged behind the US by a decade and the Netherlands lagged by two.
Meanwhile, in Colombia, the coverage achieved in 1938 stood at a level (61%) that had been achieved about half a century earlier in Europe. If we consider sewerage systems and water closet coverage (Table 1, panel B), inequalities are even larger: in Colombia, only 42% of towns with over 15,000 inhabitants had some access to modern sewerage around 1940. Although we cannot pinpoint exactly when the gap between industrialised countries and Colombia, and probably other low-income countries, started widening, Table 1 suggests that this must have happened before 1900.
Health consequences of piped water and sewage disposal systems
What was the impact of sanitary infrastructures on health outcomes? I compare studies using econometric analyses and find that infant mortality rates declined between 9% and 20% and deaths due to waterborne diseases between 22% and 25% after the improvements in water supply. These size effects are quantitatively significant, although smaller than initially shown by the landmark study by Cutler and Miller (2005).
What explains the limited effects of piped water? In the absence of efficient systems of waste disposal, the effectiveness of waterworks is impaired by inappropriate storage and removal of human excrement, leading to higher exposure to enteric diseases. Piped water could be easily contaminated where there is rapid urban growth and overcrowding, as well as additional pollution caused by the discharge of wastewater from factories.
The health impact of public health interventions can also differ substantially across contexts. For instance, high rates of breastfeeding and higher inequality decrease the impact of waterworks. Environmental conditions can be important too, since temperatures and humidity influence the mobility and survival of pathogens and vectors. Access to piped water and sewers has the potential to provide greater community protection from the seasonality of certain diseases. Finally, the effectiveness of waterworks also depends on technical considerations, such as their ability to supply a constant service. Overall, this evidence points to the need for more detailed knowledge of local contexts to understand their interplay with public health measures.
Drivers of investments in waterworks and sanitation
I study the determinants of spending on waterworks and sewerage with, to the best of my knowledge, a new framework that distinguishes between proximate and ultimate factors à la growth economics (Gallardo-Albarrán and Inklaar 2021, Rodrik 2003). Proximate drivers refer to inputs of production that are easily observable and required to offer sanitary services, such as physical and human capital. In contrast, ultimate drivers operate indirectly and over a longer time frame via supply or demand forces. In this column, I focus on ultimate drivers.
Institutions
Do more democratic institutions lead to greater investment in sanitary infrastructures? Certainly, this may have been the case in some contexts, such as the US where women’s enfranchisement led to higher public health spending, but it is far from a universal pattern. In England, the extension of franchise did not always lead to greater public health spending, due to resistance to greater taxation by different groups of voters. In Germany, on the other hand, the rising income of industrialists, who had significant political power in local elections, and factory needs were key drivers of local water demands. Therefore, self-interested elites could lead to sanitary reform, if this was in their interest.
In other world regions, colonial influence shaped the long-run evolution of public goods provision. In India, the British created differences in historical property rights by setting up different colonial revenue systems. Areas where this was transferred from cultivators to landlords performed worse in the 1980s than places where taxes were collected from peasants, although the landlord system was abolished in the 1950s. In Africa, on the other hand, there is no clear-cut colonial ‘legacy’. Colonies varied greatly in their capacity to levy taxes, healthcare spending, and the number of civil employees in the medical and sanitation departments.
Biogeography
The availability of abundant water, soil type and orography posed real constraints to municipalities that often struggled to find suitable and sufficient amounts of water in a context of rapid population growth. In Bombay and Singapore, burying water mains – a practice imported by engineers from England to prevent freezing during cold months – soon became a problem as the pipes would severely rust in about two decades or less.
The historical literature also often cites pestilence, and cholera in particular, as a driver of water and sanitation investments. Since the international spread of this disease in the 19th century, outbreaks wreaked havoc among populations throughout the world, potentially triggering political reaction and providing impetus for infrastructural improvements. While these may be compelling arguments from a humanitarian point of view, the literature would benefit from additional evidence from quantitative studies examining the occurrence of an epidemic and subsequent urban reform, including why earlier epidemics might not have had the same effect.
Culture
Culture as a mechanism has not received much attention from economic historians, although a number of qualitative works indicate their importance in some contexts. For instance, better medical knowledge – due, in part, to the steady increase in human capital and the teaching of hygienic ideas in schools – led to increased demand for sanitary services by both households and policymakers during 19th-century Europe.
Establishing waterworks could also sometimes be opposed on cultural grounds. In India, riots broke out in 1892 after new waterworks were constructed on the banks of the River Ganges. Similarly, discriminatory social norms could lead to major inequalities that hinder widespread access to clean water: ‘untouchables’ were often not allowed to access water sources used by higher castes.
Finally, cultural imitation and aspiration could be a positive force for installing waterworks. In Istanbul, the alla franca way of life was highly valued among the upper class in Istanbul, who were eager to adopt Western technologies that represented modernisation.
Conclusions
Three patterns are crucial in the global unfolding of the sanitary revolution between ca. 1850–1940. First, major cities throughout the world built these infrastructures at a (roughly) similar time, between ca. 1850s and 1890s. Second, there were large differences in their timing, both within and between countries before ca. 1880; afterwards, only municipalities in some (industrialised) countries converged with the frontrunners. And third, the within-city diffusion of pipes and sewers was even more unequal between countries than the initial construction of waterworks and sewerage. Future research should employ a more comprehensive basis to solidify these findings.
When studying the health consequences of new water and sanitation technologies, we should pay much more attention to the conditions that make sanitary reforms succeed or fail. A research agenda in this direction includes extending our analyses to other world regions and periods, including rural settings where these investments were made much later and thus the benefits may have been greater. In addition, a careful estimation of neighbourhood and regional spillover effects could shed light on the relative importance of spatial factors operating beyond the household.
On the question about the drivers of waterworks and sewerage diffusion, a satisfactory answer cannot be provided yet despite the vast body of knowledge produced in the last decades. The literature has primarily focused on economic and political considerations (e.g. funding, franchise extension, construction costs, elites’ interests), and too little attention has been paid to how these elements interact with broader biogeographic and cultural contexts.
The development of a culture of hygiene during the 19th century, ultimately underpinned by scientific medical advances, first spread among the elite and ultimately increased the perceived value of expensive public health investments. This was particularly salient during deadly epidemics, such as cholera, that were associated with filth and deprivation. The quantitative importance of this mechanism, however, is unclear, and further research is needed to assess its importance in various contexts. The literature would greatly benefit from non-Western experiences where epidemic outbreaks did not recede during the late 19th century.
Source : VOXeu








")


")



.jpeg")





















")




")








")




")
")

")




